Pulmonary Rehabilitation

The Challenge
Chronic respiratory conditions are among the most common causes of disability and hospital admission in the UK.
Pulmonary Rehabilitation (PR) is the most effective intervention for aiding people with chronic lung conditions. Yet it remains one of the most underutilised services in the NHS.
Only around 50% of eligible patients ever access PR. Waiting lists have grown significantly post-pandemic, and services face mounting pressure to deliver more with fewer resources.
People diagnosed with COPD in the UK with millions more undiagnosed
Of eligible COPD
patients never access
pulonary rehabilitation
Annual NHS cost of
COPD hospital
admissions – PR
reduces readmissions
by up to 50%
Deliver standardised group rehab programmes
A PR course typically lasts six to eight weeks with two sessions per week, each around two hours, combining an individually prescribed exercise programme with education sessions covering aerobic exercise, resistance training, and lifestyle support.
Supervised exercise groups
Schedule in-person appointmens through autonom-e with reminders, location, and instructions to prepare for each session.
Breathlessness management groups
Assign instructors, clinical specialists and assistants to support patients with supervised, tailored exercises and educational sessions
Education groups
Standard PR education topics include anatomy of the lungs and disease pathophysiology, anxiety and depression, self-management and action plans, managing breathlessness, medications and inhaler technique, managing exacerbations and chest infections, airway clearance and the Active Cycle of Breathing Technique, nutrition, pacing, and smoking cessation. These are typically delivered as weekly 30–45-minute group education sessions running alongside the exercise component, often by different members of the MDT.
Maintenance and long-term self-management groups
Prepare patients for self-management beyond discharge and schedule post-discharge follow-ups to monitor progress remotely
Your custom groups
The groups above are just a few examples you can configure in autonom-e. Alternatively, you can create your own groups, appointments and associated resources to assign as many staff and patients as needed!
How group therapy can help
A single clinician delivering an 8-week virtual group therapy programme to 10 patients generates the same throughput as 80 individual appointments — without proportional cost increases or the need to travel.
The challenge is with coordination: scheduling cohorts, capturing PROMs across groups, managing reminders, and reporting outcomes at the service level.
Autonom-e provides the digital infrastructure that makes group therapy possible and scalable whilst reducing administrative burden, improving workforce utilisation and the patient experience.
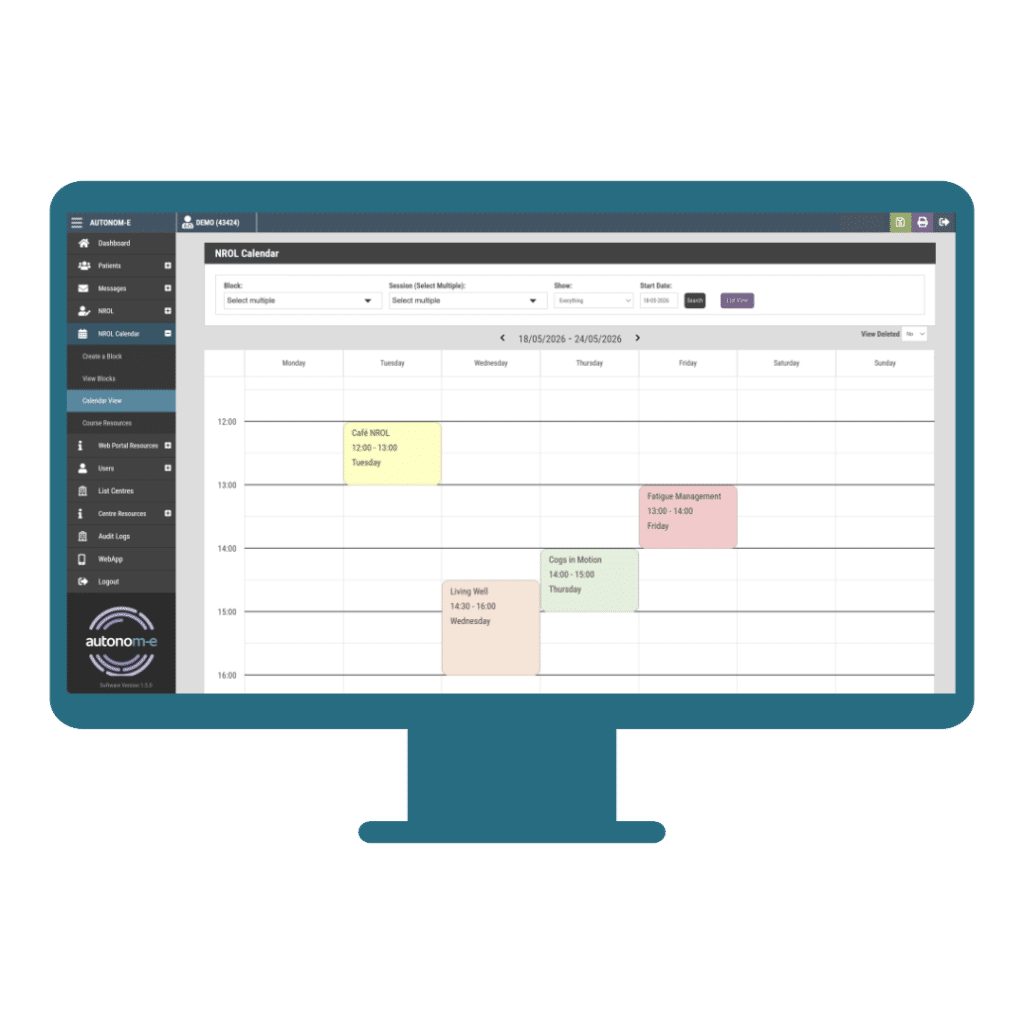
Each session is scheduled, patients are automatically notified, PROMs are captured before and after each block, and outcomes are available in real time on the clinician dashboard.
Co-ordinating group therapy
Referral & Triage
Cohort assignment
Session scheduling
Automated reminders
Monitoring & review
Discharge & PIFU
Platform Features for group therapy services
Streamlined referral, assessment & triage
Patients can be referred from primary care, from external referring teams across a region, or via self-referral if enabled.
Referrals sent directly to autonom-e are encrypted at rest and in transit.
Entry assessments can be configured for different pathways to support initial triage and stratification into group cohorts.
Pre- and post-programme PROM capture to measure group-level and individual outcomes.
Group scheduling and cohort management
Create blocks of weekly group therapy sessions in advance from the clinical dashboard. Triage patients and assign to appropriate groups based on external referral recommendations.
Assign facilitating staff & tech support to each session. Sessions automatically push to each patient’s app with date, time, format, and joining instructions.
Reporting and service analytics
Automated PROM dispatch on entry and exit of therapy programmes collects outcomes to demonstrate change in health.
Recorded attendance allows staff to monitor uptake, throughput, DNA rates, and ROI for every hour of staff time spent delivering care.
Cohort-level outcomes dashboards showing improvement trends across group programmes. Individual patient progress visible within the group context. Export clinical reports directly to electronic health records (e.g. SystmOne).
Service-level data to support commissioning decisions, business cases, and NICE compliance reporting. Cost-effectiveness modelling data to demonstrate value to ICB commissioners.
Self-management and resources
Configurable digital resource library aligned to each group programme (condition-specific written, audio, and video content). Signposting to peer support, local services, and third-party providers within the app.
Translatable resources supporting diverse and multilingual populations. eDiary tools for symptom tracking, goal-setting, and exertion monitoring between sessions
Why choose autonom-e for group therapy?
01
Configurable to your pathway
Tailor group programme structures, eligibility criteria, PROM bundles, session formats, resources, and branding to match your service design – without expensive bespoke development.
02
Reduces administrative burden
Appointment scheduling, automated PROM capture eliminate paper, postage, and manual data entry. 1,250+ estimated clinical admin hours saved each year in Lancashire.
03
Reduces waiting times
Group therapy enables services to multiply appointment availability with the same staff time, allowing for waiting times to be cut and pre-appointment administrative tasks to be automated.
04
Scalable across organisationstions
Deploy autonom-e in a single-service or multi-site deployments across ICBs, NHS Trusts, community providers, and VCSE organisations – with each site maintaining its own configuration and branding.
05
Evidence ready
Capture group-level and individual outcomes data to evaluate service impact, demonstrate cost-effectiveness to commissioners, and support research bids or NICE submissions.
06
Improved health equity
Increased rehab provision and workforce utilisation enables patients to receive more intensive and multi-disciplinary care remotely from home, without the need for travel.
Outcomes
90%
reduction in time spent supporting screening
83%
Reduction in clinician time on virtual assessments (Airedale & Bradford)
96%
PROM completion rate across patient cohorts (Airedale & Bradford)
Contact Us
For general enquiries, sales and technical support, get in touch!
Follow us: